Patello-Femoral Joint Pain

Your Physiotherapist has diagnosed you with anterior knee pain also known as patello-femoral joint pain (PFJP). What now? This information page is designed to help you in addition to the advice given by your physiotherapist. By following these exercises, we will guide you through each step on your return to activities of daily living or sporting goals you have
Any exercise has an inherent risk. If you have any queries we would advise you to consult with your physiotherapist.
What is the Patello-femoral Joint?
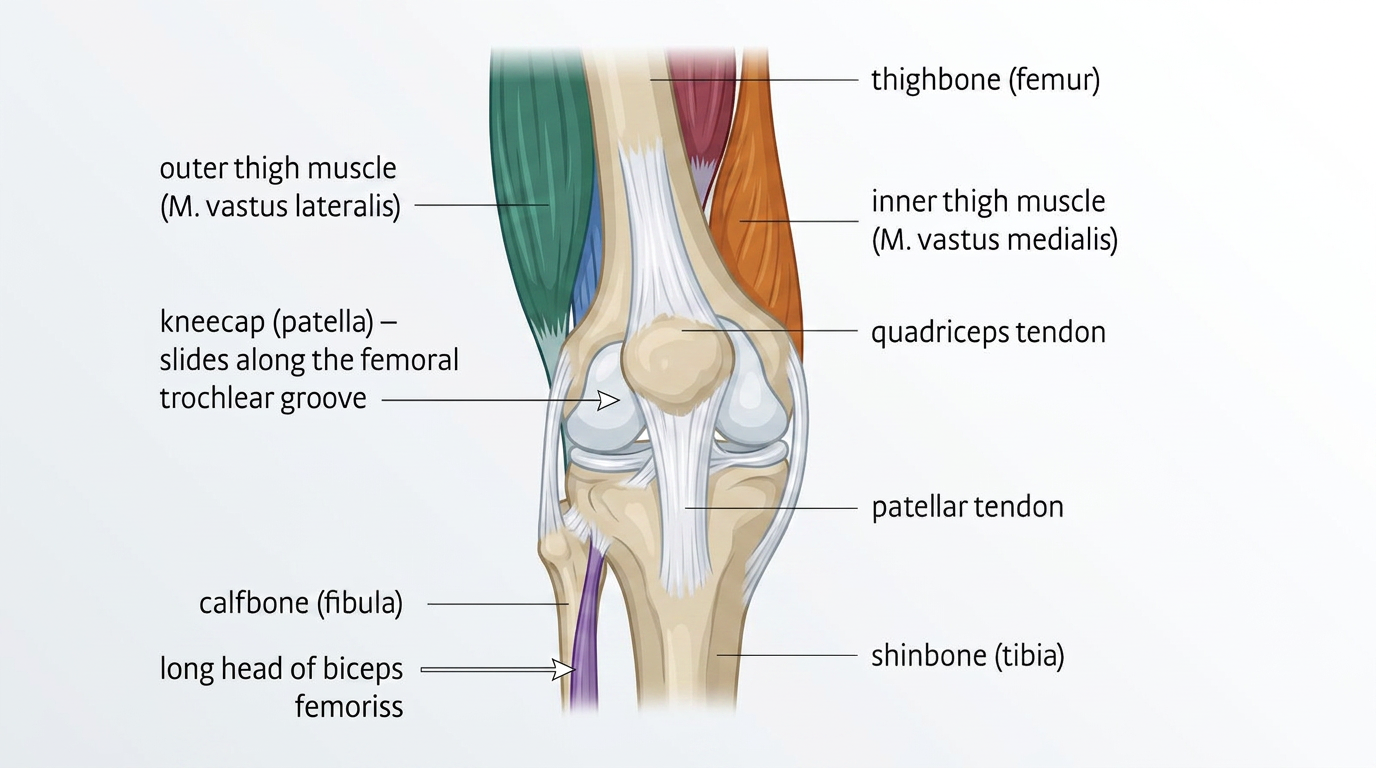
The Patello-femoral joint is formed between the knee cap (patella) and the thigh bone (femur).
The knee cap sits in a small groove on the femur called the trochlea.
A number of muscles attach to the knee cap providing movement at the knee and help stabilise it within the trochlea to provide smooth pain free movement.
-
There are numerous names for PFJP:
Anterior Knee Pain
Patella Mal-tracking
Chonromalacia patellae
Runners knee
Patello-femoral joint syndrome
There is no specific cause for your PFJP, however it generally is related to altered or overloading at the joint due to various reasons:
Strength
The quads are the big muscles at the front of your thigh. Pain at the knee cap can limit how well they work and cause weakness. This can affect the movement of the knee cap and how you carry out your daily activities or sports. You may experience further irritation at the knee however not damage. Looking above the knee, the gluteal muscles, or your bottom muscles, control the movement of your thigh bone (femur). Weakness at these muscles can affect control of single leg movements like going up and down stairs, walking or running.
Overload
Your body will have a level of activity that is normal to you and your knee is happy to accept that level. When you rapidly increase, or vary that load it can cause overload. This can be a good thing; however, it can cause an increase in sensitivity at the knee especially if you don’t allow enough rest or the excessive load irritates weak structures around the PFJ.
Biomechanics
You may have heard your physiotherapist talk about altered biomechanics at your knee when you perform some activities. They may also have discussed an increased valgus movement when you bend your knee in standing. This is when you try a squat type movement and your knee moves inwards.
This can cause pain at the PFJ, however, ensuring you have strong muscles above, at and below the knee can help control the movement at the knee and reduce the irritation.
-
Physiotherapy is the best and most effective method to help manage your pain and help you return to your normal function. Your physiotherapist will help you identify any issues through their initial assessment and will help you with a specific individualised exercise program.Your rehab plan may aim to address the overload at the patella-femoral joint by:
Reducing pain
strengthening weak structures (above and below the knee)
Correcting the way you move
Improving your movement control
Stretching tight structures
To achieve your specified goals as discussed with your physiotherapist, you will be required to attend regular physiotherapy appointments and most importantly continue your exercise program at home.
-
After an injury you may have heard from someone before about RICE (rest, ice, compression and elevation) when managing an injury. However, rest can be harmful and inhibits recovery. Recent research has now advised we use the acronym POLICE.
Protection
Optimal-Load
Ice
Compression
Elevation
The key term is Optimal-load, this replaces Rest. You may need to speak to your physiotherapist to discuss what your optimal load might be as it is specific to you but will help speed up your recovery process.
Flare ups
An increase in pain or ‘flare up’ is common with PFJP. The key is to manage this effectively and efficiently. By using POLICE this can help reduce the initial pain. During a flare up manging your optimal load is important. You may need to reduce the stresses at the PFJ, reduce the amount of exercises and daily activities that you do. Over time gradually increase your activity back to previous levels. You can discuss optimal load with your physiotherapist.
-
Unfortunately, there is not definite answer to this question. There are no quick fixes and it requires active participation from the patient throughout the process.
We would, however, expect to see improvements within 3-6 months especially if the patient continues to maintain their specific exercise program. Most people will return to their pre-activity levels including sports.
The Exercises
Participating in an exercise program carries a certain element of risk for some people. You should consult with your physiotherapist before initiating this program to ensure your safety.
If you have any issues please do not hesitate to contact the physiotherapy department. If you feel light headed, dizzy or have issues with your breathing please contact your general practitioner (GP) immediately.
When carrying out this exercise program you may feel some discomfort at your knee. It is important that this pain does not exceed 3/10, where 10/10 is the maximal and 0/10 is no pain.
Level 1
Rehabilitation aims to gently activate the muscles above and around the knee in a controlled way that supports and protects the joint without increasing pain. The exercises should feel challenging enough to stimulate adaptation and recovery, but not so demanding that they irritate the PFJ. As the gluteal muscles have a strong impact on the forces at the PFJ, these exercises target them specifically to help reduce pain and improve the forces going through the knee.
Clam with band
In side lying with your knees bent to 90°, in line with hips and a band around both knees.Raise the top knee away from the bottom knee without rotating at your pelvis or spine.
Perform 3–5 sets of 45-second holds, resting 30–60 seconds between sets.
Hip abduction/extension with band
In side lying have your bottom knee bent to 90° and the top leg straight, with the band around both knees. Lift your top leg up and back without rotating your pelvis or spine.
Perform 3–5 sets of 45-second holds, resting 30–60 seconds between sets.
Fire hydrant with band
On your hands and knees with the band above both knees. Bring your leg back with your heel towards the sky and turn your knee outwards.
Perform 3–5 sets of 45-second holds, resting 30–60 seconds between sets.
Wall Sit
Perform 3–5 sets of 45-second holds, resting 30–60 seconds between sets.
Isometric Knee Extension
Level 2
Level 2 challenges the muscles more whilst still ensuring pain levels are kept low. The aim is to also start working the muscles while you move and should be challenging enough to achieve muscular adaptation without causing overload and pain the to the PFJ.
Box Squats
Side Plank Clam
In side lying with your knees at 90 ° in line with your hips and elbow directly under your shoulder. Raise your pelvis up into a partial side plank position and raise the top knee away from the bottom knee without rotating at your pelvis or spine.
Perform 3-5 sets of 45 second holds, resting 30-60 seconds between sets.
Crab walks
Perform 3-5 sets of 45 second holds, resting 30-60 seconds between sets.
Step up (medium)
Level 3
Level 3 focuses on developing motor control and progressing your exercises, so the muscles work effectively during movement. Rather than simply building strength, this stage retrains the brain and body to coordinate the correct muscles at the right time. By consciously engaging muscles with good movement quality, you build better control, stability and confidence through the knee as activity levels gradually increase. The exercises should feel challenging enough to stimulate adaptation and recovery, but not so demanding that they irritate the healing tissues. Modify and vary your exercises by working similar muscle groups but in ranges or positions that do not cause significant increases in pain. E.g. use a higher box/seat to do a box squat.
Goblet Squat
Weighted Lunges
Cross Over Step Up
Kettlebell Romanian Deadlift