Hip Dysplasia

You have been diagnosed with hip dysplasia, what now? The aim of this webpage is to help you understand this diagnosis and we will guide you through each step on your return to normal activities or any sporting goals you may have, whether you have surgery or not.
-
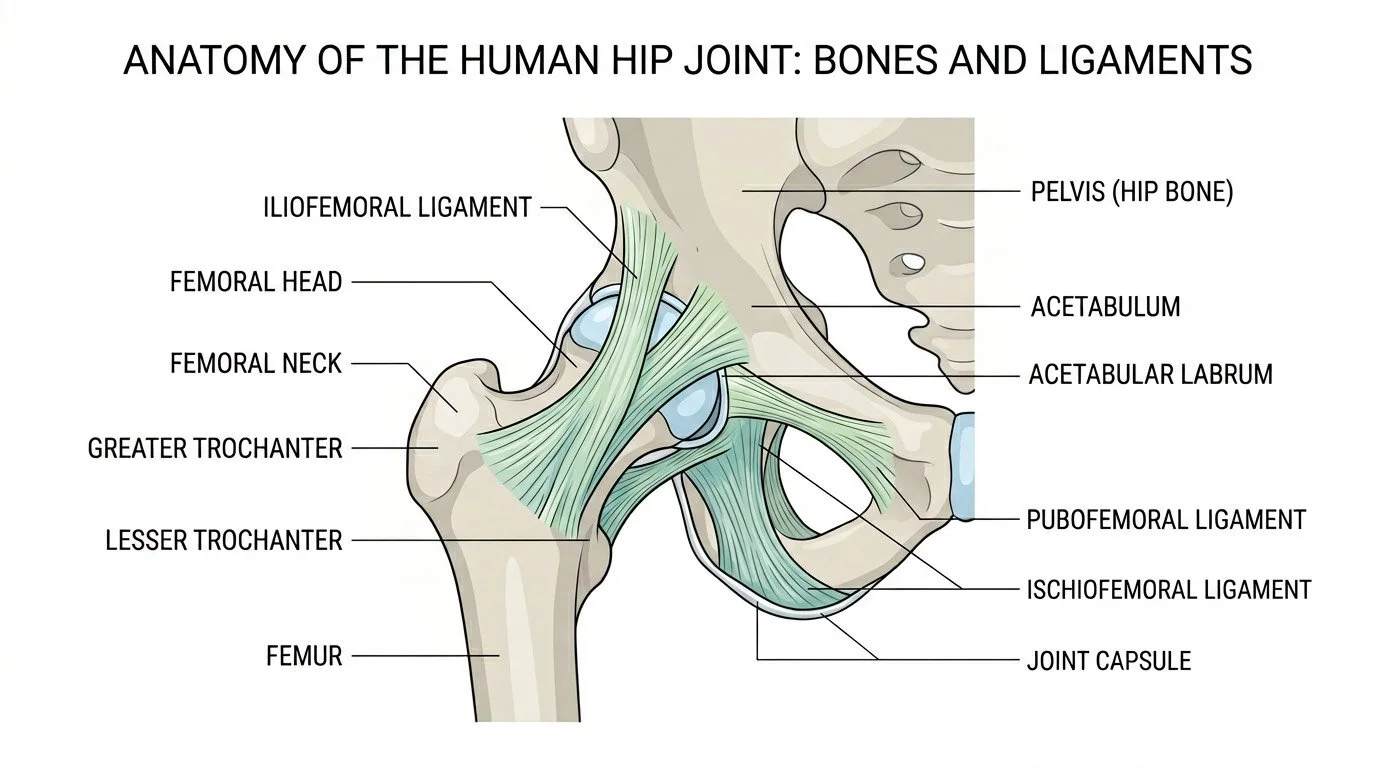
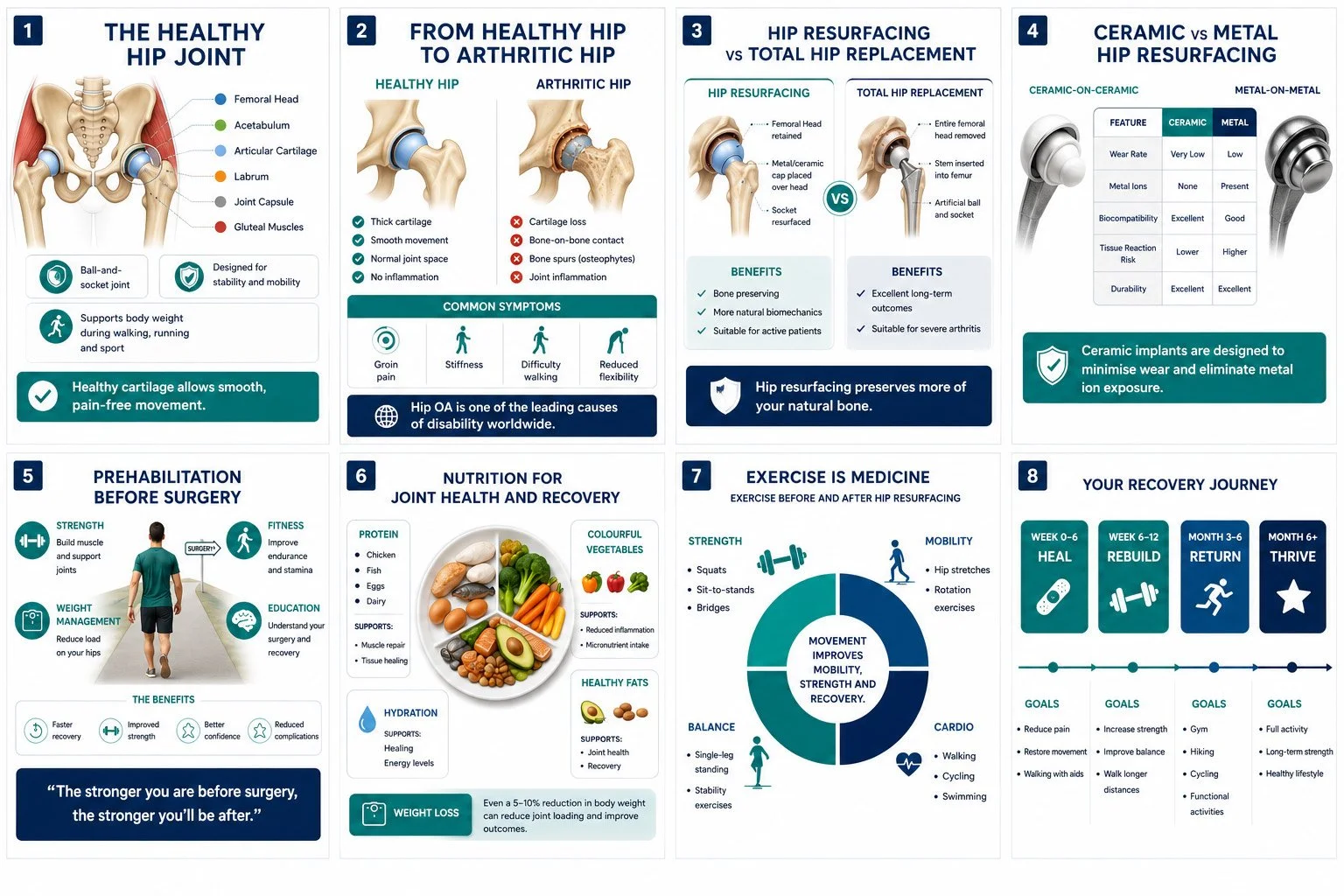
The hip is a ball and socket joint.
The ball (femoral head) is the rounded top of the femur, commonly known as the thigh bone.
The socket (acetabulum) is located in the pelvis.
The femoral head fits into the socket. The ball-and-socket anatomy allows the leg to move forward, backward and side to side. It also allows for internal and external rotation (pointing the toes inward and outward).
Cartilage helps stabilise the joint and facilitates hip movement.
Articular cartilage: Both the femoral head and acetabulum are lined with a strong, slippery material called articular cartilage. This cartilage allows the surface for the ball and socket to glide against each other during hip movement.
Labrum: Another piece of cartilage, called the labrum, rings the outer edge of the acetabulum. The labrum deepens the socket, making the hip joint more stable, and its elasticity allows for flexibility.
Having an understanding of hip anatomy is necessary to understand hip dysplasia and why you may need a PAO.
-
If you find yourself with hip dysplasia as a young person or adult you may have had a previous diagnosis as a baby. This is called Developmental Dysplasia of the Hip (DDH). It is sometimes known as ‘clicky-hips’ or ‘loose hips.’ You may have had treatment such as a pavlik harness or plaster cast or surgeries as an infant or child and have residual hip dysplasia now. However, you may not have had an infant diagnosis. Your symptoms might have started developing as a teenager or young adult after exercise or prolonged standing.
-
The reasons why some cases of Hip Dysplasia are not picked up until later in young adult life are not fully known. One reason could be due to the fact that our current screening methods for Hip Dysplasia in infants don’t pick up every case. Another theory is that some forms of hip dysplasia develop during a growth spurt in adolescence and are linked to ligament laxity (hypermobility syndromes).
-
The causes of hip dysplasia still remain much debated and further research is required. However, there are some known risk factors that may play a part:
First born
Female gender Breech presentation
Swaddling as a baby
The heritable component of DDH due to common genetic links is approximately 55%. (links with GDF5 gene)
Ligament laxity or hypermobility syndromes, or a family history of this – 47% more prevalent in DDH 10 Hip Dysplasia in teenagers & young adults
-
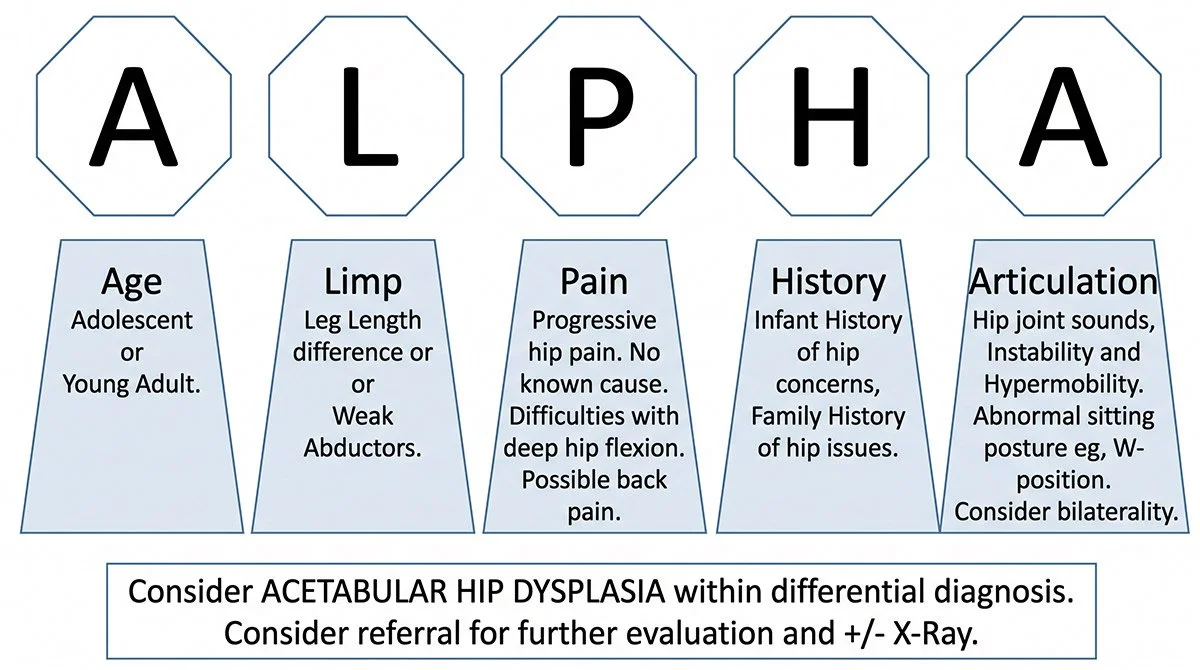
It is not uncommon for people to find it takes a long time to find a clear diagnosis of hip dysplasia, the average time to diagnosis is 5 years. Dysplasia often masquerades as other issues such as tight muscles and there are no specific clinical tests that diagnose dysplasia. You may have found you have seen a medical professional or Physiotherapist who has treated these other issues initially but that it has not helped your symptoms. It is important that you see a Physiotherapist and Consultant who specialises in dysplasia.
Pregnancy, relationships & family life
-
It is fine to get pregnant if you have hip dysplasia. Extra weight carried through pregnancy will increase the load going through the hip joints, which may increase your pain.
If you have hypermobility, your hip pain can increase during pregnancy as the hormone relaxing increases ligament laxity in preparation for the birth- this results in less stability from the ligaments around the hip joints and can cause increase shearing and therefore pain. Physiotherapy, maintaining strong muscles and pelvic corsets can help with this.
If you have had a pelvic osteotomy, this surgery does not encroach the birth canal and therefore you can deliver normally if you wish.
-
Hip dysplasia is approximately 12 x more likely when there is family history. If you have a diagnosis of hip dysplasia it is important that your new-born child has an ultrasound screening. (International Hip Dysplasia Institute).
-
Being intimate with your partner is a key part of your relationship but your hip pain may make you worried or anxious about this. The most important thing is to be honest with your partner about what is painful and uncomfortable. Positions that force the hips into extreme movement and full flexion may be more painful. Keeping your core stable, with your feet on something will provide improved joint position sense and reduce unstable feelings
-
Receiving a diagnosis of hip dysplasia can be overwhelming. You might feel sad, angry, uncertain of the future or even relieved to find out what is wrong. All these feelings are normal. It’s important to know that you are not alone, there are many others with this condition, and seeking support (see final page for support groups), coping strategies & practical tips from others can be really beneficial, whatever treatment you decide on.
It can also take a while for information about your condition to sink in. You may want to save this webpage to refer back to. You can find details of online support networks & further resources at the bottom. If you have chosen to undergo surgery then talking to others with hip dysplasia can help you feel prepared for what to expect and what recovery will be like.
One of the most important things in the journey of hip dysplasia diagnosis is acceptance of the diagnosis and then moving forwards.
If you are on social media, there are some great pages to help you. The HIPDYSPLASIAPHYSIO online and Instagram is one excellent site, with excellent help.
If you are not having surgery you can skip to the pre – operation exercise section,
Modifying Your Lifestlye
You may find that modifying your lifestyle helps you manage your hips on a day to day basis, in the following ways:
Maintaining a healthy weight Nutrition/dietician input
Stopping smoking – Smoking significantly affects bone healing if you are considering surgery- this is vital
Staying active with low-impact exercise such as swimming (front crawl) or cycling. Breastroke can sometime irritate pain, but everyone is different
Making adjustments at work
Evidence shows that weight loss through exercise and a healthy diet may reduce your pain and improve your general lifestyle. Losing weight also helps improve your mood, reduces inflammation in the body, can lead to improved sleep and reduces the risk of other diseases.
Although you have been listed for a PAO it is vital that you get ready for it both physically and mentally. By doing this your outcome will be much better. A regular routine of varied exercise, including; strengthening, flexibility and cardio vascular fitness is essential.
Prehabilitation & Conservative management
Hip dysplasia prehabilitation is all about preparing the hip, pelvis, and surrounding muscles for the demands of treatment or surgery. By improving glute strength, core control, hip stability, mobility, and movement confidence, we can help reduce compensatory patterns and support better post-operative recovery. Prehab also gives patients the chance to understand their condition, learn how to move safely, and build confidence before surgery, which can make the early stages of rehabilitation feel less daunting. A tailored, progressive programme can play an important role in helping patients feel stronger, more informed, and better prepared for their recovery journey.
-
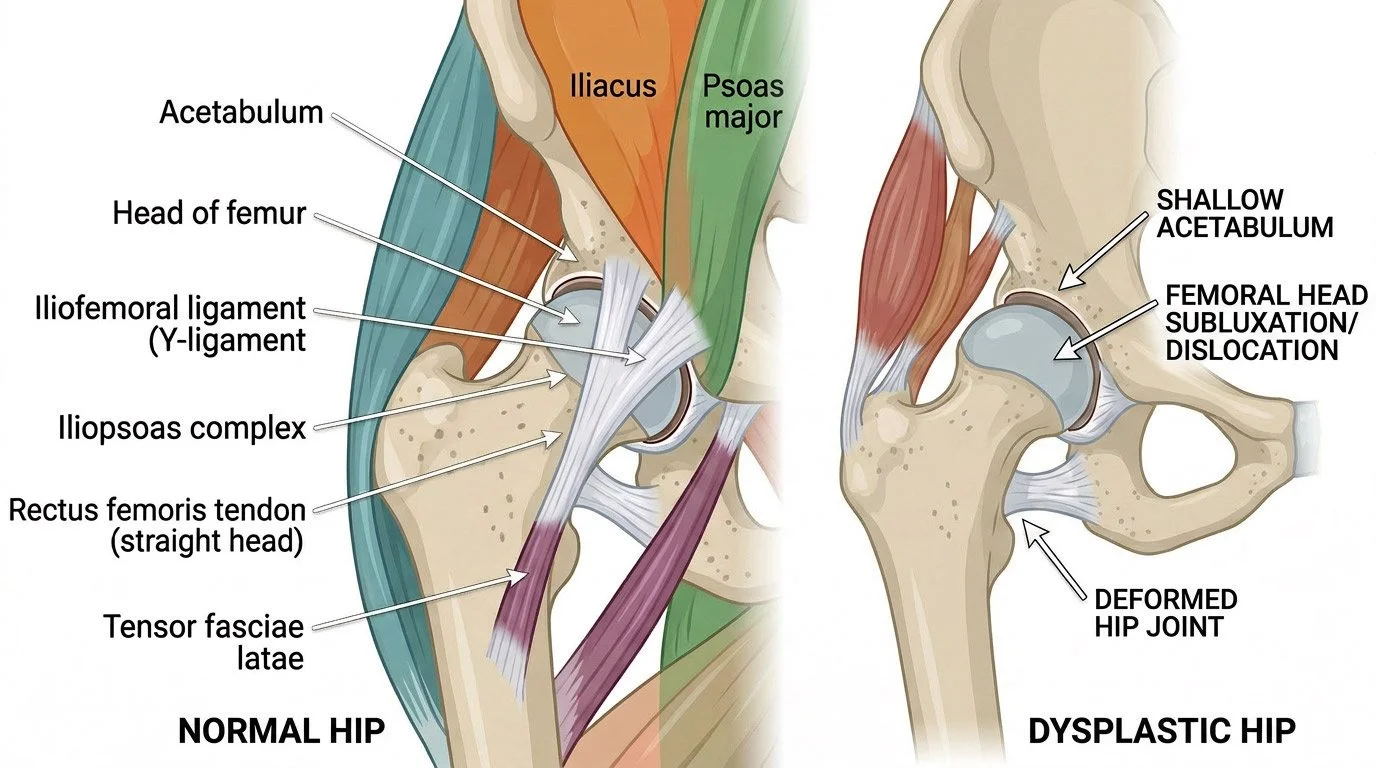
A periacetabular osteotomy (PAO) is a surgical procedure to treat a congenital hip condition called hip dysplasia. Hip dysplasia is either present from birth or develops in the first few months of life. Patients suffering from this condition have a shallow socket (acetabulum) of the hip joint.
This causes misalignment of the head of the thigh bone (femur) in the acetabulum and leads to premature wear and tear of the joint over the years. Patients usually start experiencing pain in the groin region at 20 to 30 years of age with symptoms of limping, waddling or walking on their toe.
The diagnosis is confirmed by an X-ray of the hip joint. An MRI scan may be ordered to check the condition of the labrum and bony surfaces.
-
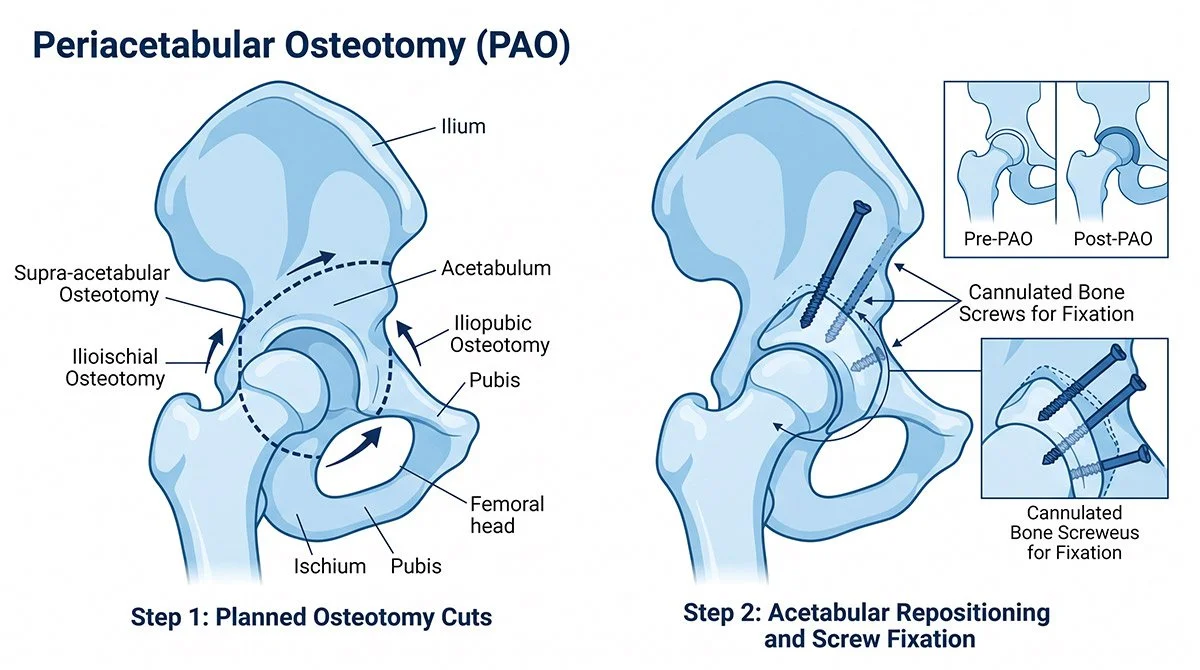
The operation of is designed to move the socket (acetabulum) of the hip joint so that it covers more of the femoral head (ball). The aim is to improve the biomechanics of the hip joint and reduce the high stresses that start to cause damage and arthritis because of the shallow acetabulum.
The operation involves a series of bone cuts around the acetabulum, freeing it from the pelvis and allowing it to be moved to a new position; it is then fixed in place with 2 – 3 screws. The bone usually takes 6-8 weeks to heal, however it can take 6 months to one year to achieve optimal function. Functional outcome is heavily dependent upon the pre-operative condition of the hip joint and any Pre-existing change and arthritis of the hip can have a significant negative affect upon functional outcome.
“You will not cause any further ‘damage’ to yourself by participating an exercise program, however if you do have any concerns please liaise with your consultant or physiotherapy team. By developing further muscular strength you will not only improve you outcomes post-surgery but also protect your joint following surgery by providing a form of shock absorber. ”
Below is a varied exercise plan that may help you; some exercise positions may need to need altered to reduce your hip pain but achieve maximal muscle effort. When exercising there is likely to be an element of pain, however the aim is not to exceed 3-4/10 where 0/10 is your base line. You should however find the exercises difficult and strenuous on the muscles, approximately 7-8/10 where 10/10 is maximal effort.
Strength Program: Upper Body

Pick 2 exercises from either a push or pull movement pattern. Push exercises include press ups, bench press and shoulder press. Pull exercises include lateral pull downs and rows (of any type). The definition of strength is the ‘ability to produce a maximal force’ therefore to improve strength, aim to work at a higher intensity and lower volume. E.g. 1 – 5 repetitions, 4 – 5 sets with 3 minutes rest between sets.
Core
Front Plank
The aim is to work hard. With the planks hold for 5 – 10 seconds, repeat 5 times and do 3 sets. You can make this harder by holding for longer. With the pall off press, repeat 10 – 15 times, doing 3 sets.
½ Side Plank
The aim is to work hard. With the planks hold for 5 – 10 seconds, repeat 5 times and do 3 sets. You can make this harder by holding for longer. With the pall off press, repeat 10 – 15 times, doing 3 sets.
Pall-Off Press
The aim is to work hard. With the planks hold for 5 – 10 seconds, repeat 5 times and do 3 sets. You can make this harder by holding for longer. With the pall off press, repeat 10 – 15 times, doing 3 sets.
Lower Limb
Double Leg Bridge
Lying on your back with your knees bent and band around your knees. Squeeze your bottom muscles and tighten your stomach muscles. Lift your bottom off the bed until there is a straight line between your shoulders and knees. Keep your knees apart against the resistance of the band. By keeping your feet flat, digging your heels into the floor you will increase the activity in your hamstrings. Then on elevation, imagine there is a nut between your buttocks which you are trying to crush.
Hold for 5 – 10 seconds, repeat 5 times, 3 sets
Goblet Box Squat with band
With a band around your knees, select an appropriate weight and hold up to your chin in front of you. Perform a squat as far as you feel comfortable, by sitting back, keeping your knees over your second toes, with your back straight and body weight evenly spread over both feet. You can make this easier by doing this movement from a chair but on elevation, imagine there is a nut between your buttocks which you are trying to crush.
Repeat 10 times, completing 3 sets, build to 15 times and 3 sets
Step up (medium)
Stand facing a step of appropriate height. Put your injured leg on the step and step up, bringing the other leg through at a right angle. Keep the movement as controlled as possible with your knee tracking over your second toe.
Repeat 10 times, completing 3 sets, build to 15 times and 3 sets
As these exercises get easier or become less painful, you can start to do more strength-based exercises.
Cardiovascular Program
Your cardio vascular fitness is very important and can sometimes be forgotten about
Cardiovascular exercise, or simply cardio, encompasses activities that elevate your heart rate and deepen your breath. From running and cycling to swimming and dancing, these dynamic exercises harness the power of movement to essentially prompt your body into an energised rhythm, promoting a state of health and vitality.
Cardio exercise can help control blood pressure, reduce blood sugar levels and help you maintain a healthy weight. Furthermore, Cardio exercise is a natural mood elevator. That’s because it triggers a surge in serotonin, the “feel-good” hormone that boosts feelings of happiness and well-being. Moreover, cardio can significantly enhance sleep quality, which in turn can drastically improve mental health.
-
Intensity and frequency matter: Not all cardio exercise has to be high-intensity. In fact, low and medium-intensity cardio can yield substantial benefits. For optimal results, aim for about 150 minutes of moderate-intensity exercise or 75 minutes of high-intensity activity per week.
Exercise choice: Different types of cardio are suitable for different individuals, and what works best for you depends on your health and fitness goals, current fitness level and any physical conditions or injuries you may have. For instance, if you have any issues with your joints, you might find low-impact cardio like swimming or aqua aerobics more to your taste.
Family fitness: Incorporating cardio into family activities can turn exercise into a fun bonding experience. Whether it’s a weekend bike ride, a family dance-off or a nature hike cardio activities encourage fitness and family bonding simultaneously.
Warm-up and cool-down: The importance of proper warm-up and cool-down routines cannot be overstated. These crucial stages prepare your body for cardio and help it recover afterwards, reducing the risk of injuries and enhancing your overall performance.
Hydration and nutrition: Staying hydrated and fuelling your body with the right nutrients before and after a cardio workout can drastically impact your energy levels and recovery.
Swim – bike – cross trainer
By accessing your local gym this will create a pathway for you to speed your recovery up post-surgery. Although we may not all like the gym, if we aim to return to activities such as walking, gardening, and other demanding activities the gym is a great way to condition you, to get back to these things quickly and safely.
-
The main aim following surgery is to manage pain (ensure adequate pain relief) and reduce the risks of post-operative complications, to ensure the procedure heals optimally.
Your physiotherapy team will try and get you up and moving on the day of surgery. It is normal to feel nauseous and dizzy following this procedure due to the anesthetic and severity of the procedure.
You will be partial weight bearing or advised to place no more than twenty kilograms of your weight through your operated leg. You should be encouraged to walk with a normal gait pattern using crutches with the help of your physiotherapy team, ensuring that you are safe to go home.
They will also start you on an exercise program to initiate movement of the hip and begin low level muscle activation exercises of your core and operated leg.