Anterior Cruciate Ligament: Reconstruction (ACL – R)

Anterior Cruciate Ligament (ACL) tears are a common injury, particularly among individuals involved in sports. This page is designed to support your recovery by providing clear, structured guidance—whether your treatment involves surgery or not.
By following the recommended exercises, you will be guided safely and progressively through each stage of rehabilitation, helping you return to everyday activities and achieve your specific sporting goals as efficiently as possible.
Any exercise has an inherent risk. Always consult with your physiotherapist for any queries or issues.
The Knee
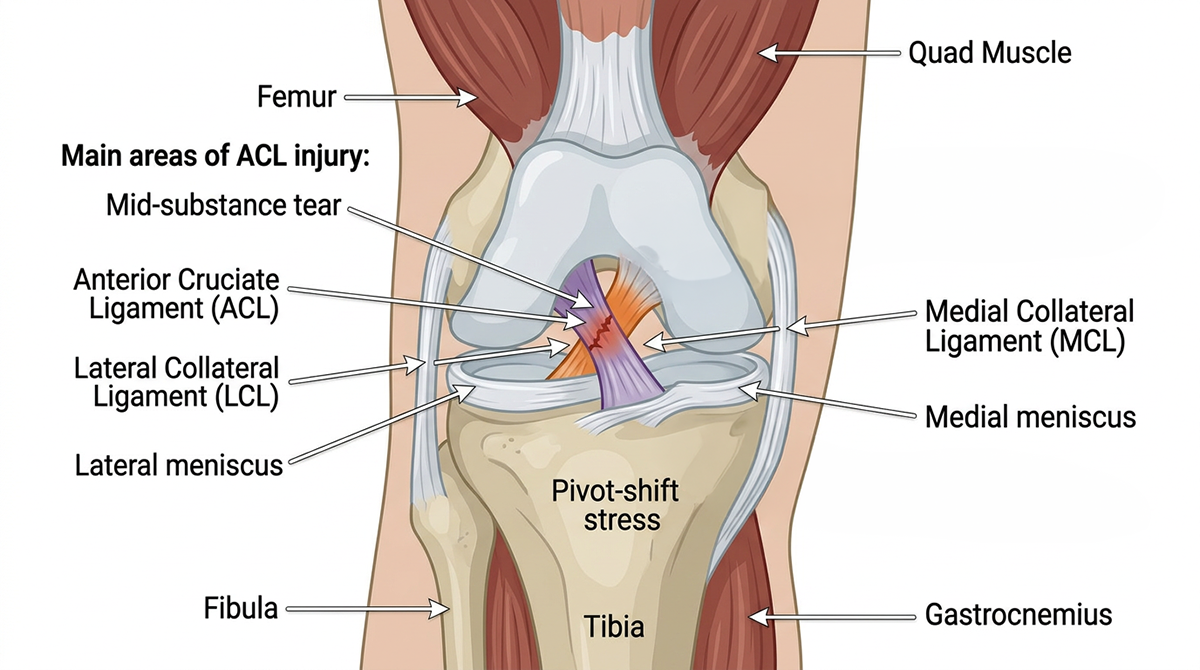
The knee is formed of the tibia (shin bone), femur (thigh bone) and the patella. To provide stability at the knee there are various ligaments. The collateral ligaments provide stability to each side of the knee and the Cruciate ligaments prevent the tibia sliding forwards and back in relation to the femur.
The ACL is a broad thick band which stops the tibia sliding forwards in relation to the femur. It starts from the bottom of the femur, and passes down and forwards to attach to the top of the tibia. As the ACL is situated inside of the joint capsule, when you rupture your ACL it causes bleeding. This is why your knee quickly swells after the rupture.
The surrounding quad, hamstring and calf muscles also play a vital role for additional stability and providing strength and movement at the knee.
-
Non Contact
Believe it or not, the most common cause of ACL injury is through a non contact mechanism when the knee is subjected to sudden deceleration forces combined with rotation eg twisting on a fixed foot, especially on pivoting and landing. Another common mechanism is through Extreme hyper-extension and hyper-flexion.
Contact
injuries occur when there has been a direct blow to the outside of the knee or lower leg. Following your injury, you may experience symptoms of giving way and instability at your knee. This may in turn affect your normal activities and participation in sport.
-
To treat an ACL injury a decision will be required as to whether you follow the surgical or conservative pathway. Not everyone needs surgery! Current research has shown there to be little or no difference, in return to activity, between surgical patients and those who choose the conservative route. It depends on various factors, including; your age, degree of your knee stability, any associated injuries such as meniscal tears and the level of activity/sport that you wish to return to. An in depth discussion with your physiotherapist and consultant will help you with your decision.
Despite your decision initial management of ACL sprains remains the same.
Treating an ACL injury involves deciding between a surgical or conservative (non-operative) approach—and it’s important to know that surgery is not always necessary. Current research shows little to no difference in return-to-activity outcomes between those who undergo surgery and those who follow a structured rehabilitation programme.
The right option depends on several factors, including your age, the stability of your knee, the presence of associated injuries (such as a meniscal tear), and the level of activity or sport you aim to return to. A detailed discussion with your physiotherapist and consultant will help you make an informed decision that suits your goals and lifestyle.
Non-operative rehabilitation
Many individuals can achieve a good level of function through physiotherapy alone, without needing surgery. This approach may involve modifying or avoiding high-impact sports and activities that involve twisting movements over the long term. However, if you continue to experience knee instability or are unable to return to your usual activities, reconstructive surgery may be recommended. ACL reconstruction is a well-established procedure that can effectively restore knee stability and support a return to sport.
Rehabilitation for all patients
Regardless of the pathway you choose, the early stages of ACL management are the same. Building strength is key—stronger muscles lead to better outcomes, whether or not you proceed with surgery.
If you are opting for a non-operative approach, follow the link to our modified strengthening programme. These exercises are also used as “prehabilitation” for those preparing for surgery, helping to optimise recovery and long-term results.
-
After an injury you may have heard from someone before about RICE (rest, ice, compression and elevation) when managing an injury. However, rest can be harmful and inhibits recovery. Recent research has now advised we use the acronym POLICE.
Protection
Optimal-Load
Ice
Compression
Elevation
The key term is Optimal-load, this replaces Rest. You may need to speak to your physiotherapist to discuss what your optimal load might be as it is specific to you but will help speed up your recovery process.
If you are not getting surgery, you can skip the next section, however it may be of interest to read, in case you are still considering this option.
-
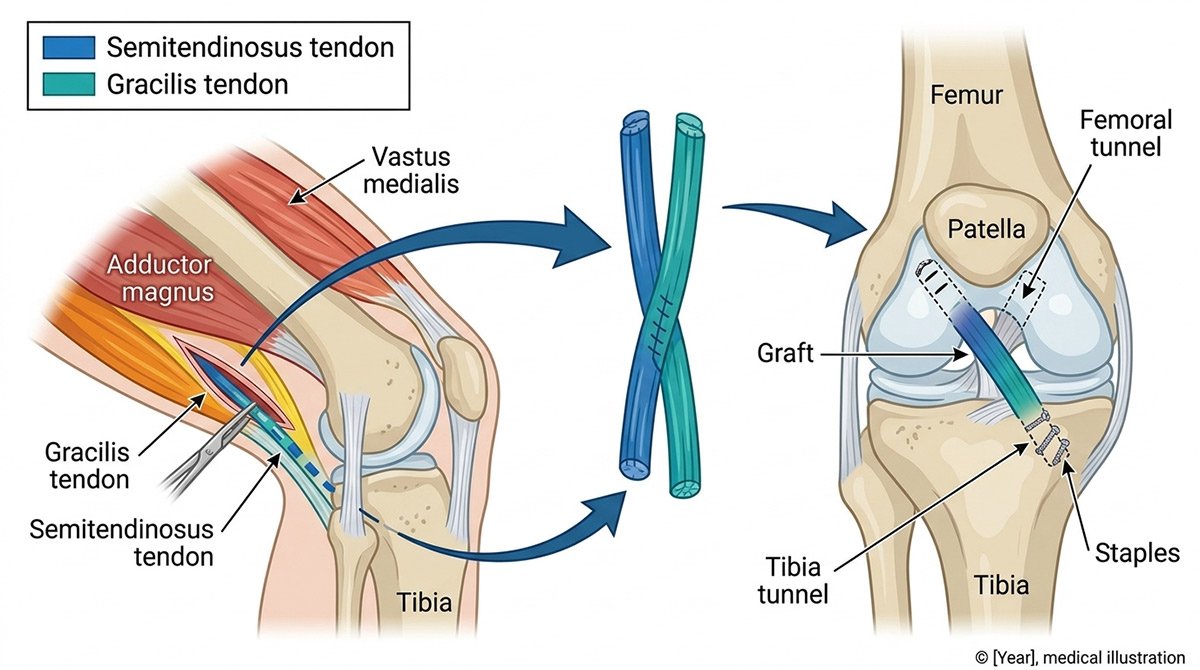
The two most common forms of ACL reconstruction are by using a hamstring or patella tendon graft. The hamstring graft is a much more common procedure which comprises of removing part of the semitendinosis and/or the gracilis muscles from the hamstrings, which are then stitched together to make the graft. Small tunnels are then drilled in the femur and tibia so the graft can then be pulled through and secured in place. The graft is placed as close to the original ACL position as possible and acts as a substitute for the damaged ACL.
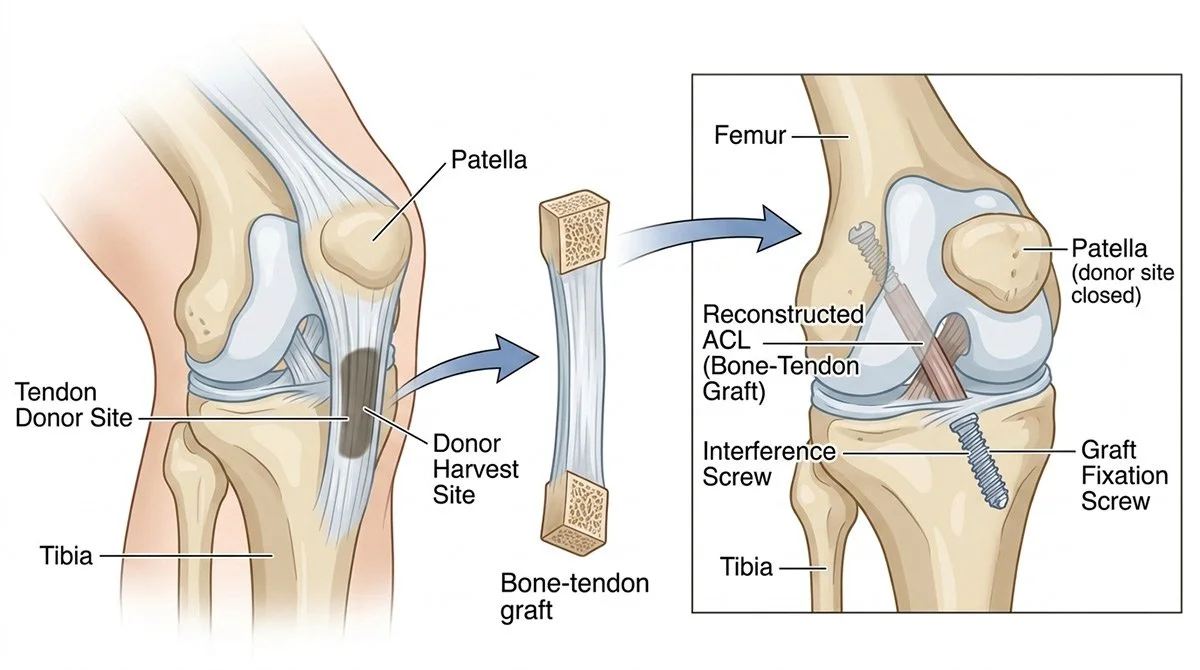
Bone Tendon Bone (BTB) Graft
Another method to fix the ACL is with a patellar tendon graft also known as a “bone-patellar tendon-bone” graft or BPTB graft, as it consists of tendon and bony attachments.
ACL reconstruction with a BPTB graft can be stronger than the hamstring graft, although there is a risk of anterior knee pain (Patellofemoral joint pain), due to where the graft is taken from. It is usually surgeon preference for which surgical procedure is used, however you can discuss this further with them.
-
LET - lateral extra-articular tenodesis
LET, or lateral extra-articular tenodesis, is a surgical procedure that is often performed in conjunction with ACL reconstruction to address persistent knee instability, particularly rotational instability. During the procedure, a strip of the iliotibial (IT) band is taken from the outer side of the thigh and rerouted under the lateral collateral ligament to the side of the femur.
Why it is performed
To reduce re-tear rates: Studies suggest that combining LET with ACL reconstruction can lower the rate of the new graft tearing.
To improve stability: It helps control rotational movements of the knee, which are often a problem after ACL injuries.
For specific patient groups: It may be particularly beneficial for young athletes returning to high-risk sports or in cases where a previous ACL reconstruction has failed.
Meniscal Repairs
Meniscus repairs are common with ACL tears, with meniscal lesions being associated with 41–55% of ACL ruptures. When a tear is repairable, surgeons often perform a concurrent meniscus repair during the ACL reconstruction to improve stability and help prevent future osteoarthritis. The success of this combined approach depends on factors like tear type and location.
-
Improved knee stability: A torn meniscus can compromise knee stability, and repairing it provides a more stable joint.
Protection against arthritis: Repairing the meniscus helps protect the joint cartilage from further damage and can help prevent the early onset of osteoarthritis, which is a risk with an unprepared meniscus.
Gold standard for certain tears: For specific types of tears, like bucket-handle tears, concurrent repair with the ACL reconstruction is considered the gold standard.
-
Combined recovery: A combined surgery may increase the overall recovery time and rehabilitation period. Most meniscal repairs prevent squatting for 3 months post surgery.
Tear type and location: The success of a meniscus repair depends on the tear's size, type, and location within the meniscus. Some tears are not repairable and may require a meniscectomy (removal of the torn part) instead.
Surgical technique: The specific surgical technique used can influence the outcome, with various methods like all-inside, inside-out, and others being used based on the injury.
If you have any questions about your surgery, talk to your surgeon, their team and your physiotherapist. The more you understand, the more informed decision you can make about whether or not to have surgery or continue with conservative care.
-
Following surgery you will experience a certain amount of pain, this can be controlled by taking regular pain medication as prescribed by your doctor.
At this point the POLICE principal will take place. Ice not only helps to reduce swelling but can also help manage acute post-operative pain. Following the surgery you will be allowed to fully weight bear, unless instructed otherwise by your consultant. It is important to continue mobilising your knee and maintaining as normal a walking pattern as possible. Your physiotherapist will teach you how to use crutches to ensure you are optimally loading the knee is the safest possible manner. They will also give you exercises to do, which are available below.
You are likely to be discharged home on the same day as your surgery, as long as you are safe to do so.
-
As with any surgery there is a risk of possible complications.
These include:Wound infection, including MRSA – infections are very rare and usually
around the skin. Occasionally, deep infection may occur in or around the
knee joint. The risk is rare; less than 0.1%, that is less than one person
out of one thousand.Tender red scar – this is rare also and normally resolves over a period of
a year.Stiffness can be an issue following knee surgery and your physiotherapy
is very important, especially regaining full extension (straightening) of
the knee.The surgery fails or the ACL re-ruptures resulting in ongoing instability.
This occurs in approximately 3-7% of cases and can often require further
surgery with a revision reconstruction.Risk from the anaesthetic – your anaesthetist will talk to you about this.
Risk of numbness which is fairly common next to the scars on the knee. Rarely the surgery can cause a nerve injury which could cause weakness and numbness to part of the knee and/or leg.
All operations carry a small risk of pain syndrome. All lower leg surgery caries a small risk of deep vein thrombosis (DVT) and pulmonary embolus (PE) these can be very serious and potentially fatal. The risk is very low and early weight bearing and mobilisation with physiotherapy help to counteract this.
It is important to note should you experience any severe redness and increased temperature around the knee to contact your GP as soon as possible. Another post op complication can be the risk of Deep Vein Thrombosis, therefore if you are experiencing any intense severe calf of groin pain, you will need to contact your GP or attend accident and Emergency urgently.
-
Following surgery you will experience a certain amount of pain, this can be controlled by taking regular pain medication as prescribed by your doctor.
At this point the POLICE principal will take place. Ice not only helps to reduce swelling but can also help manage acute post-operative pain. Following the surgery you will be allowed to fully weight bear, unless instructed otherwise by your consultant. It is important to continue mobilising your knee and maintaining as normal a walking pattern as possible. Your physiotherapist will teach you how to use crutches to ensure you are optimally loading the knee is the safest possible manner. They will also give you exercises to do, which are available below.
You are likely to be discharged home on the same day as your surgery, as long as you are safe to do so.
It is important to note should you experience any severe redness and increased temperature around the knee to contact your GP as soon as possible. Another post op complication can be the risk of Deep Vein Thrombosis, therefore if you are experiencing any intense severe calf of groin pain, you will need to contact your GP or attend accident and Emergency urgently.
-
Prehabilitation
What is prehabilitation?
Most people are familiar with rehabilitation—the exercises and treatment used to restore movement and strength after an injury or surgery. Prehabilitation applies the same principles, but focuses on the period before surgery.The aim is to optimise strength, mobility, and circulation in your knee ahead of your operation, giving you the best possible foundation for recovery. One of the most important goals at this stage is regaining full knee extension (the ability to fully straighten your leg), as this can significantly influence your post-operative progress.
Why is prehabilitation important?
Before anterior cruciate ligament (ACL) reconstruction, an effective prehabilitation programme should include:
Quadriceps strengthening
Improving range of motion
Balance and proprioception (joint awareness and control)
While programmes may vary in length and content, research shows that prehabilitation can lead to improved range of motion and quadriceps strength for at least six weeks after surgery—and potentially much longer. A well-structured and consistent programme may also help reduce the risk of re-injury or injury to the opposite knee following ACL reconstruction.
Starting your rehabilitation journey early can make a meaningful difference to both your short-term recovery and long-term outcomes.
Prehab Exercises
Range of motion
Static quad and opposite leg lift
Flex on wall
Strength Training Guidelines
Strength is typically defined as the ability to produce maximal force. Traditional strength training programmes often involve low repetitions (1–5 reps), multiple sets (4–5), and longer rest periods (around 3 minutes), performed up to three times per week.
However, meaningful improvements can also be achieved with moderate-intensity training. Performing 8–12 repetitions for 3 sets, three times per week, can still lead to effective muscle strength and adaptation.
Following a significant injury, pain and tolerance levels can vary. It’s important to choose a training approach that feels manageable and appropriate for you. Your programme should challenge you, but remain within a level that allows consistent, controlled progress without aggravating symptoms. Choose exercises specific to you and the adaptations you want to achieve, but vary so they don't cause too much pain, which can cause muscle inhibition.

Box Squats
Leg Press
Step Up
Bridge
RDL