Knee Osteoarthritis

Osteoarthritis is a normal age related condition that causes joints to become painful and stiff. The knee is one of the joints most affected by osteoarthritis. The aim of this webpage is to provide you with information about the problems faced with age related changes in your knee and suggest a few helpful hints on how to help manage your symptoms.
-
The knee is one of the largest joints in the body. It acts as a hinge and withstands a lot of twists and turns in our everyday life. If you are active and play sport, you will need your knee to be as strong as possible to meet your sporting demands.
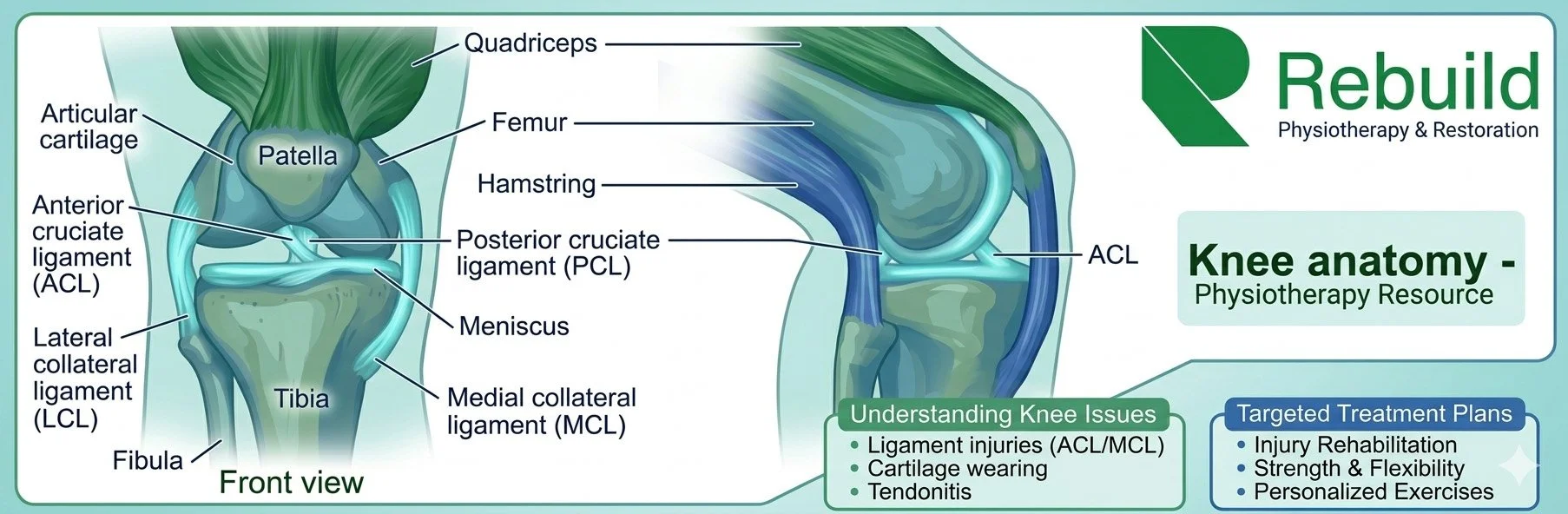
Bones
The knee joint is formed by three bones – the thigh bone (FEMUR), the large shin bone (TIBIA) and the knee cap (PATELLA). The smaller shin bone (FIBULA) is also closely linked, but is not part of the knee.
Ligaments
Four large and strong ligaments keep the knee joint stable, two outside the knee joint (MCL/LCL) and two inside (Cruciates ACL/PCL).
Cartilage
There are also two cartilage structures, also known as Menisci, inside the knee which help to keep it stable and provide some shock absorption.
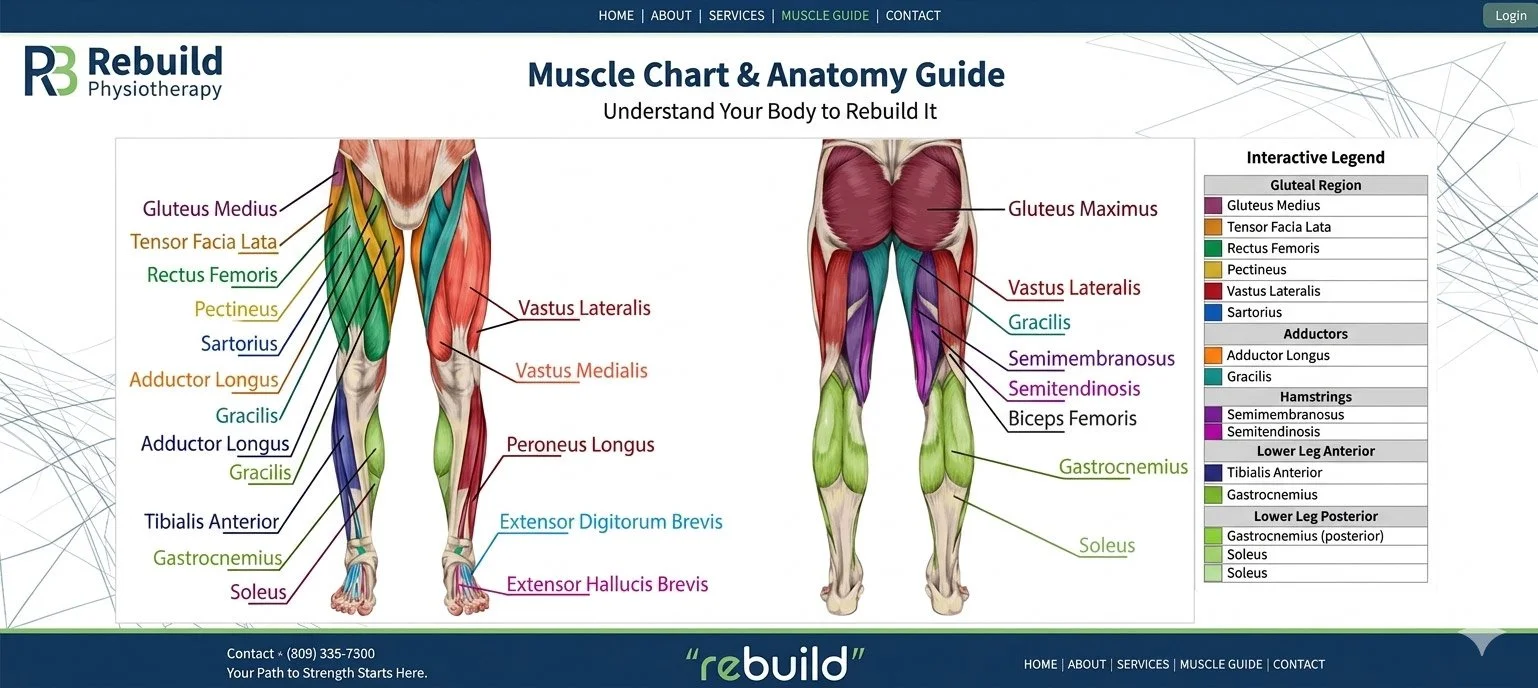
Muscles
To provide movement at the knee, muscles attach to the bones by strong connecting tissues called tendons. These muscles also provide further support and can also reduce the forces going through the knee. These muscles are:
The Quadriceps (at the front of the thigh)
The Hamstrings (at the back of the thigh)
The Gastrocnemius and Soleus (large Calf muscle)
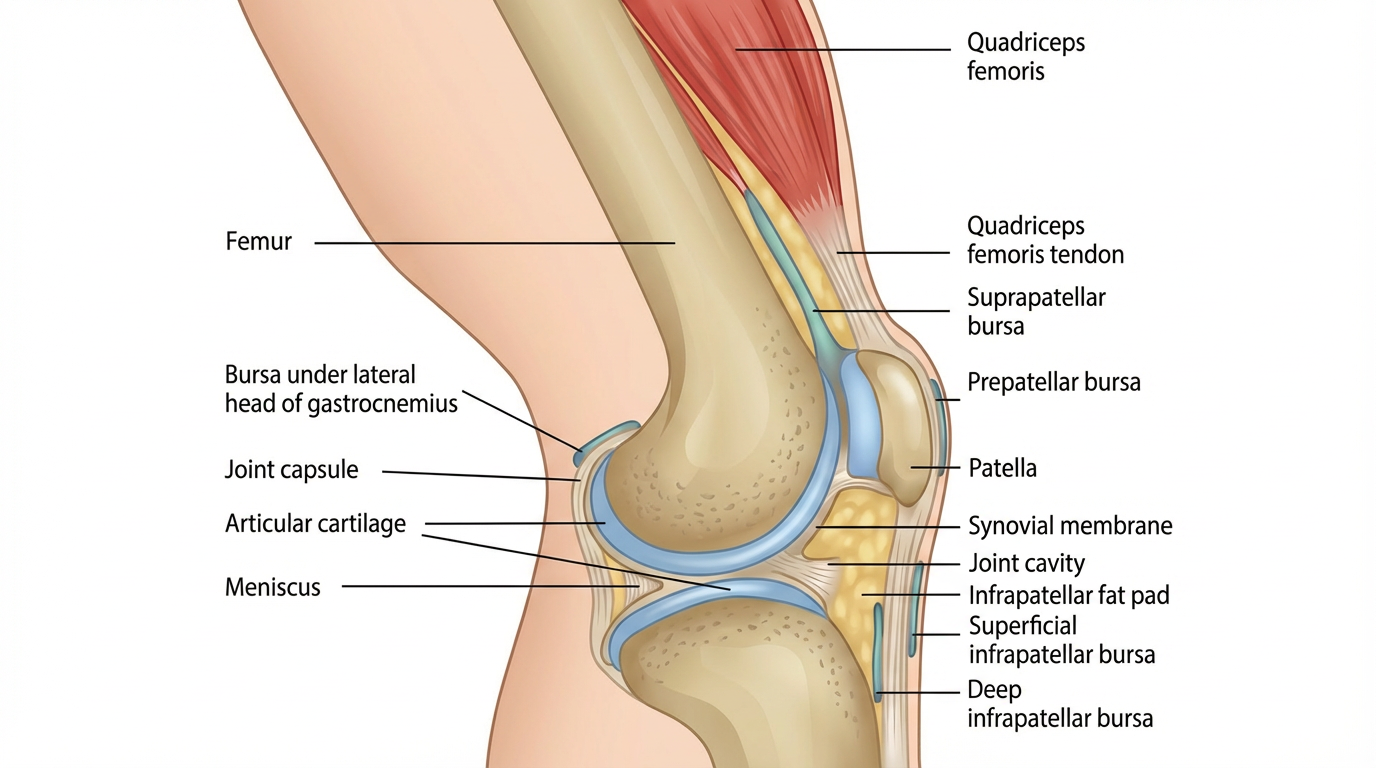
Joint capsule
Each joint also contains synovial fluid, which acts as lubricant to reduce friction as we move. The more we move, the more synovial fluid is distributed across the joint surfaces lubricating the joint, and also explains why we stiffen up if we keep still for too long.
-
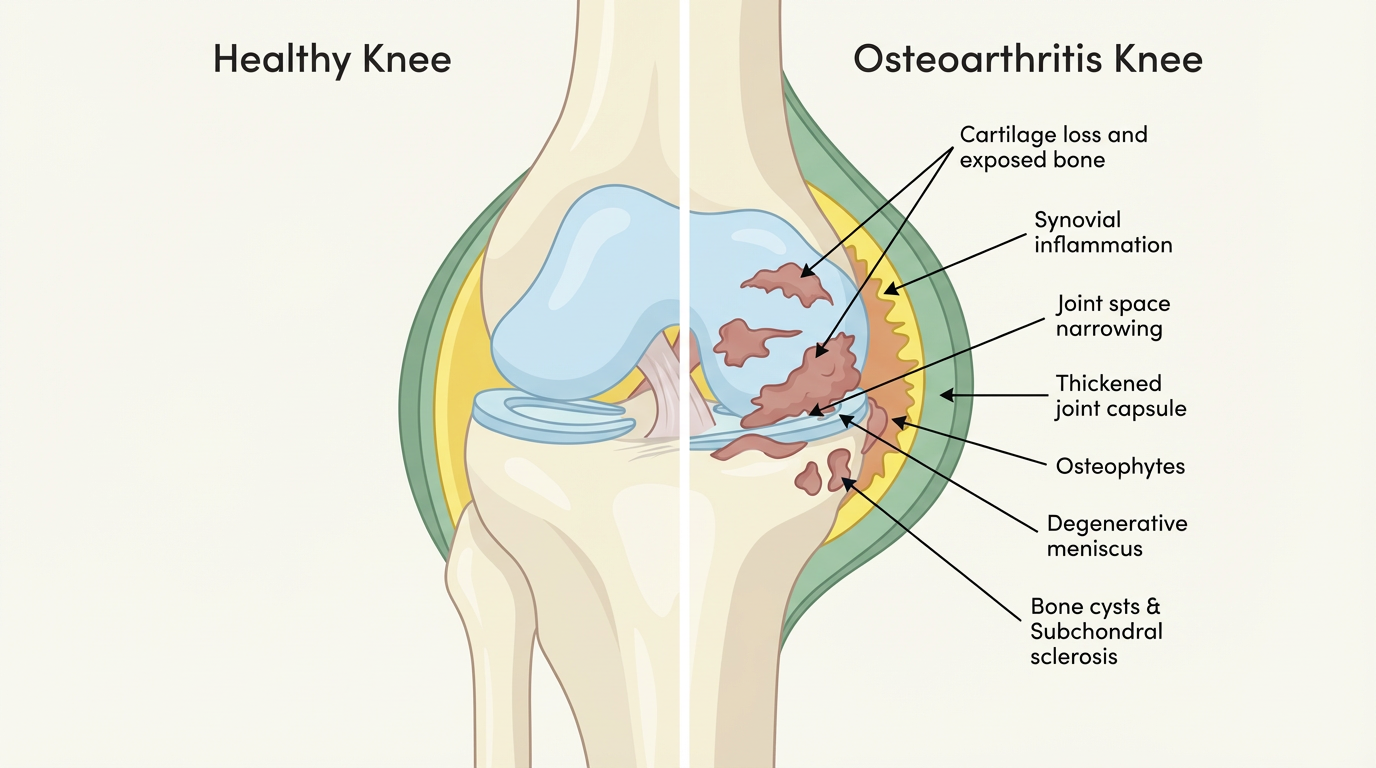
Osteoarthritis is a normal age related change that occurs in the joints. When a joint develops osteoarthritis, it affects the cartilage covering the ends of the bones and can cause the development of bony spurs called osteophytes. Additional changes occur to the synovial fluid, causing stiffness in the joint and occasionally the joint space begins to narrow which can further reduce the movement of the joint.
These changes in and around the joint are partly the result of the inflammatory process and partly your body’s attempt to repair the changes which have occurred.
This process is a perfectly normal part of ageing and happens in all joints but tends to happen earlier in joints that carry a lot of weight through them. This is why the knee, and also the hip, are most commonly affected. In many cases there is no pain, however, as this process continues it can increase symptoms of stiffness and pain to become more severe and persistent.
-
The symptoms of osteoarthritis can include:
Pain
A grating or grinding sensation when the joint moves (crepitus)
Swelling (either hard or soft).
Sometimes the knee may either lock or give way when you put weight on it.
Weakness and wasting of the quadriceps muscles at the front of your thigh
Loss of range of motion, particularly when bending and straightening the knee
Stiffness around the knee, making movements slower or more difficult.
Trouble going up stairs. Changes to the knee’s range of motion may change a person’s natural gait while climbing stairs.
A loss of balance. Balancing on the affected leg may be more difficult than balancing on the unaffected leg.
Limping. In moderate to severe cases of knee OA, knee pain and other symptoms may cause a person to find walking difficult and can lead to a limp. It is important to try and avoid limping, to allow the joint to move through its full natural range of movement.
-
Almost anyone can get osteoarthritis, but it’s most likely if:
You’re in your late 40s or older. Remember it is a normal age related change to the joint surface.
You’re overweight: Being overweight is an important factor in causing osteoarthritis, especially in the knee. It also increases the chances of osteoarthritis becoming progressively worse.
You’re a woman: twice as common in woman as in men.
Your parents, brothers or sisters have had osteoarthritis
You’ve previously had a severe knee injury: repetitive activity or physically demanding jobs can increase the risk. Previous injuries to the ligaments or meniscus including surgery can increase the risk of arthritis.
Your joints have been damaged by another disease, for example rheumatoid arthritis or gout.
-
There are several ways you can help yourself, including:
Losing weight if you’re overweight
In fact, evidence shows that weight loss through exercise and a healthy diet may reduce your pain and improve your general lifestyle. Losing weight also helps improve your mood, reduces inflammation in the body, can lead to improved sleep and reduces the risk of other diseases.
Exercising regularly (both muscle-strengthening and general aerobic exercise)
Using painkillers (analgesics) or anti-inflammatory creams, gels and tablets.
Reducing stress on the affected joint (for example by pacing activities, using a walking stick or wearing appropriate footwear)
-
ESCAPE-pain is a rehabilitation programme for people with chronic joint pain of the knees and/or hips, that integrates educational self-management and coping strategies with an exercise regimen individualised for each participant. It helps people understand their condition, teaches them simple things they can help themselves with, and takes them through a progressive exercise programme so they learn how to cope with pain better.
Robust evaluation shows that ESCAPE-pain:
Reduces pain
Improves physical function
Improves the psychosocial consequences of pain
Reduces healthcare and utilisation costs.
-
If you still have pain after trying self-help measures, your doctor may recommend the following treatments:
Physiotherapy
Steroid injections into the painful joint
Surgery, including joint replacement.
There is minimal strong evidence to support the use of joint injections in a knee with normal age related changes, especially as the effects have a short-term effect. You should discuss this option further with your health care professional especially as there are some side effects and adverse risks involved with a steroid injection.
Recent studies have shown that in the early stages of knee OA surgery should not be used. It has frequently shown poor outcomes and in many cases has sped up the progress of the OA.
Injections
Injections for knee OA are common, non-surgical, intra-articular treatments designed to reduce pain, improve joint function, and, in some cases, delay the need for total knee replacement. They are generally used when exercise, weight loss, and oral medications (like NSAIDs) have failed to provide relief.
Here is a summary of the most common types of knee OA injections:
-
Mechanism: Powerful anti-inflammatory medication that reduces synovial inflammation.
Best For: Short-term, fast-acting pain relief, particularly during an acute flare-up of knee pain accompanied by effusion (swelling).
Duration: Relief usually lasts from a few weeks to 3–4 months (sometimes up to 6 months).
Considerations: Not recommended for long-term management due to potential for cartilage degradation with frequent, repeated use. Doctors generally limit these to 2–3 injections per year. Not to be used if listed for a knee replacement as can increase risk of infection.
-
Mechanism: Injects a gel-like substance that mimics natural joint fluid to improve lubrication and shock absorption.
Best For: Mild to moderate osteoarthritis, especially for patients who cannot tolerate painkillers or for whom steroids did not work.
Duration: Slower to take effect than steroids (4–6 weeks for full effect), but can provide relief for 6–12 months.
Considerations: Studies show mixed results regarding efficacy, with some guidelines (e.g., NICE) not recommending them, while others (e.g., OARSI) find them useful for moderate OA.
-
Mechanism: Uses a concentrated sample of the patient’s own blood (platelets) to release growth factors that promote tissue healing and reduce inflammation.
Best For: Younger, more active patients with mild to moderate OA, or those looking for a more natural approach.
Duration: Often provides longer-lasting relief (6–12+ months) compared to steroids.
Considerations: Considered more effective than HA or cortisone in the medium-to-long term, though results can vary based on preparation and injection technique. Generally considered experimental and often not covered by insurance.
-
Stem Cell Injections: Experimental technique (using fat or bone marrow) aimed at potentially repairing damaged tissue. Evidence is still emerging, and it is not typically approved for routine use.
Prolotherapy: Involves injecting an irritant (usually dextrose) to stimulate the body’s healing response. More effective than placebo for pain, but less supported by evidence than steroids or PRP.
-
Mechanism: Integrates into the synovial membrane of the knee joint, increasing its elasticity and providing a long-lasting cushioning barrier that reduces inflammation and friction.
Effectiveness: Studies show significant, long-lasting reduction in knee OA pain for up to 3 years, with some data suggesting benefits lasting up to 5 years.
Procedure: A single 6ml injection performed in an outpatient setting, often using ultrasound guidance, usually under local anaesthetic.
Recovery: Minimal downtime; patients can often walk out of the clinic and return to daily activities quickly, though high-impact activity should be avoided for a few weeks.
Side Effects: Generally safe, with common but temporary side effects like mild pain, redness, or swelling at the injection site.
-
vs. Steroid Injections: Unlike steroids, which typically offer short-term relief (under 6 months) and can damage cartilage, Arthrosamid is non-biodegradable and intended for long-term impact.
vs. Hyaluronic Acid (HA): While HA acts as a lubricant and is broken down by the body in 4–6 months, Arthrosamid integrates into the tissue and does not break down.
Clinical trials have demonstrated that roughly 80% of patients show a positive response, with significant improvements in pain and function.
Unfortunately, this is not provided on the NHS, however, is available through Mr Paul Jermin, Highly specialised knee consultant. Available at
https://arthrosamid.com/clinics/paul-jermin-medical-area-oswestry
-
No Cure: Injections do not cure OA; they are for symptom management.
Effectiveness Decreases: Over time, the effectiveness of injections may decrease as arthritis progresses.
Combined Therapy: Injections work best when combined with physiotherapy and strength based exercise.
| Summary Table of Injections | |||
|---|---|---|---|
| Injection Type | Primary Goal | Speed of Relief | Typical Duration |
| Corticosteroids | Anti-inflammatory | Fast (1–3 days) | 2–3 months |
| Hyaluronic Acid | Lubrication/Shock Abs | Slow (4–6 weeks) | 6–12 months |
| PRP | Healing/Regenerative | Gradual (weeks) | 6–12+ months |
| Arthrosamid | Cushioning/Lubrication | Moderate | 2+ years |
-
Physiotherapy, which encompasses exercise and education, is the best and most effective method to help manage your pain and help you return to your normal function. Your physiotherapist will help you identify any issues through their initial assessment and will help you with a specific individualised exercise program.
Your rehab plan may aim to address the overload at the knee by:
Reducing pain
Strengthening weak structures (above and below the knee)
Correcting the way you move
Improving your movement control
Stretching tight structures
To achieve your specified goals as discussed with your physiotherapist, you will be required to attend regular physiotherapy appointments and most importantly continue your exercise program at home.
-
After an injury you may have heard about RICE (rest, ice, compression and elevation) when managing an injury. However, rest can be harmful and inhibits recovery. Recent research has now advised that we use the acronym POLICE.
Protection
Optimal-Load
Ice
Compression
Elevation
The key term is Optimal-load, this replaces Rest. You may need to speak to your physiotherapist to discuss what your optimal load might be as it is specific to you but will help speed up your recovery process.
-
An increase in pain or ‘flare up’ is common with knee osteoarthritis. The key is to manage this effectively and efficiently. By using POLICE this can help reduce the initial pain. During a flare up managing your optimal load is important. You may need to reduce the stresses at the knee or reduce the amount of exercises and daily activities that you do. Over time, gradually increase your activity back to previous levels.
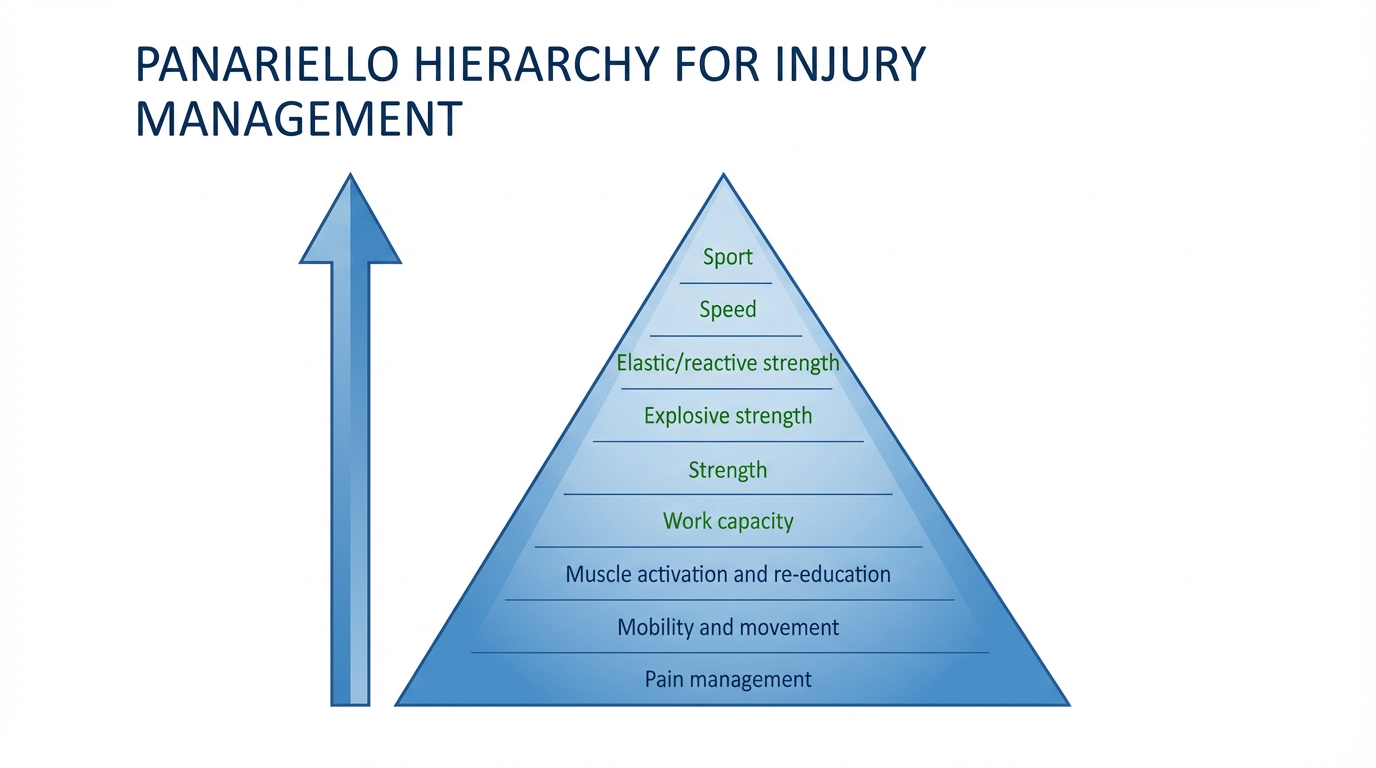
You can discuss optimal load with your physiotherapist. Below is a table which shows what type of exercises should be used and a hierarchy for return to normal activities. We will follow this pathway in the exercises later on. They often over lap and sometimes one exercise can have two goals, you can discuss this with your healthcare professional further.
-
As mentioned exercise is one of the first lines in management in a knee with normal age related changes. It is key to ensure you continue to function well by maintaining strength, range of movement, fitness and joint health with increasing evidence showing that exercise can protect the joint from further changes.
The current physical guidelines for activity in the UK are:
75 minutes of intense exercise per week
150 minutes of moderate exercise per week
2 resistance training sessions per week.
When beginning an exercise program, it’s best to start slowly. Some examples of low-impact, non-strenuous exercise include:
Stationary bike
Using a stationary bike on an easy setting allows you to slowly build your strength. Using the bike in your home allows you to avoid traffic and stop when you feel strained. A bike is a more favorable choice than walking due to the less load going through your knee. If you struggle to ride a bike, a set of home pedals is also a good option to get your knee moving.
Water exercises
Freestyle swimming provides a moderate workout. Walking in water up to your waist lightens the load on your joints while also providing enough resistance for your muscles to become stronger. This can greatly improve pain and daily function of the knees.
Yoga
Regular yoga can help improve flexibility of the joints, strengthen muscles, and lessen pain. Some yoga positions can add strain to your knees, so if you feel discomfort, ask your instructor for modifications. A class for beginners is a good place to start.
Tai chi
The slow, fluid movements of tai chi may relieve arthritis pain and improve balance. Tai chi is a natural and healthy stress reducer as well.
Walking
If you have balance problems, using a treadmill (with no incline) allows you to hold on. Walking at a comfortable pace — whether it’s indoors or outdoors — is an excellent low-impact exercise.
Muscle strengthening exercises
Once you have improved mobility and movement the next stage is to develop strong muscles to help take pressure off your knee joints and help improve balance. We will guide you through the process in the next stage of this web page.