Calf Muscle Strain

A calf injury is one of the most common injuries in sport. It occurs when you strain or ‘pull’ the muscles at the back of your lower leg. This is most often due to over stretching or overloading them beyond their limit. A calf strain often occurs during sudden, explosive movements or in sports that involve sprinting with sudden stops and starts. Although calf strains heal quickly, they are often not rehabilitated or strengthened to their optimal level. Re-injury is therefore very common and one of the biggest risk factors for a future injury is a previous calf strain.
The Calf complex (Triceps Surae)
The calf complex, medically known as the ‘Triceps Surae’, is made up of two muscles. The large gastrocnemius or calf muscle and the smaller soleus muscle. The Gastrocnemius is the more superficial of the muscles with soleus sitting beneath it.
The Gastrocnemius has two heads to it and crosses both the ankle and knee joints. This makes it somewhat vulnerable to injury. Injuries to soleus are far rarer.
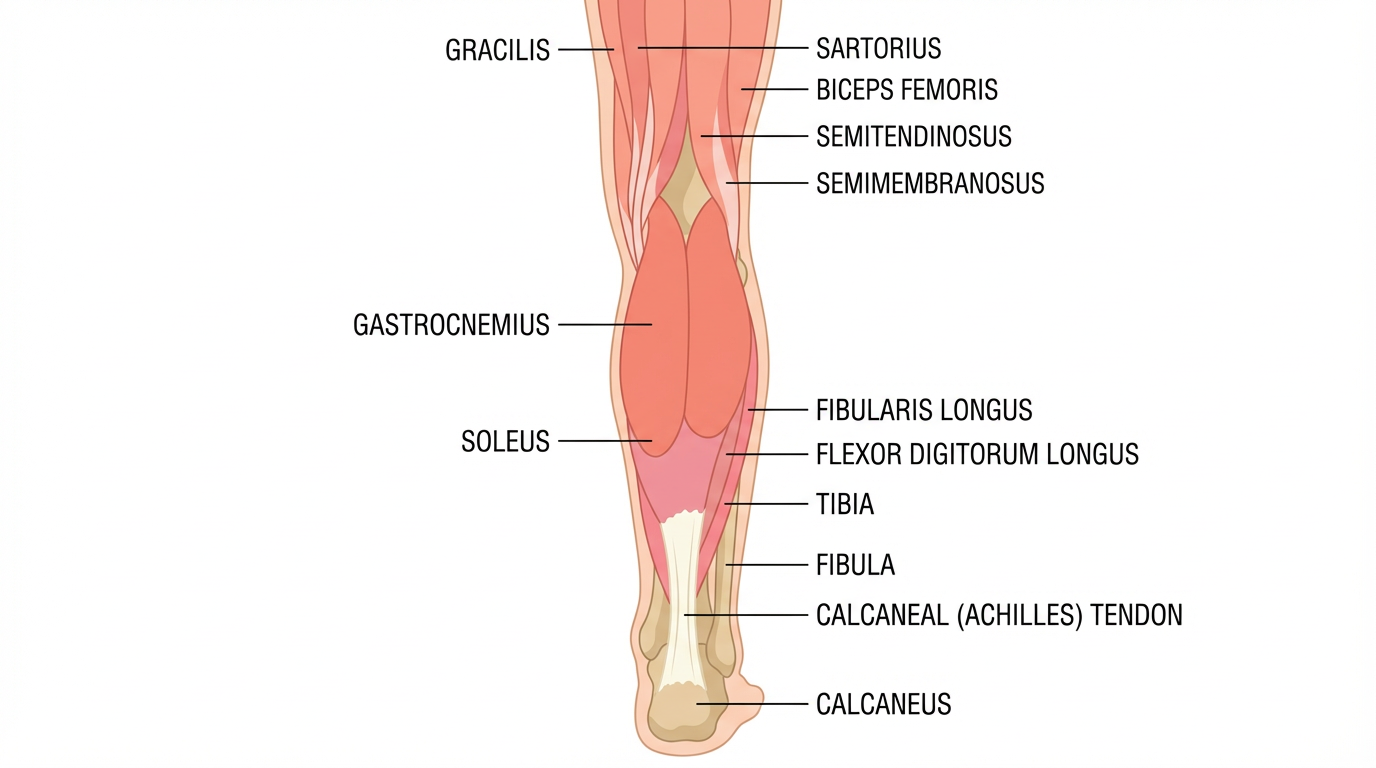
The gastrocnemius is also made up of a different type of muscle fibre to the soleus. The gastrocnemius is mainly constructed of what is known as type 2, or the explosive fast twitch, muscle fibres. Where as the soleus is made up of type 1slow twitch muscle fibres. What this means is that the soleus muscle is used mainly in aerobic activities e.g. walking, where as the gastrocnemius is mainly used for powerful actions such as sprinting and jumping.
-
A calf injury can occur if any of the tendons or muscles are stretched beyond their limit. They often occur during sudden, explosive movements, such as sprinting, lunging or jumping. But they can also occur more gradually, or during slower movements that overstretch your calf.
-
Depending on initial severity and location of your calf injury, a person can be significantly debilitated and be forced to take extensive time away from activity. Most people who suffer an acute calf strain will experience some of the following:
Sharp pain at the back of the calf occasionally accompanied by an audible or palpable “pop” and a sensation of the leg giving way.
Difficulty moving and weight bearing. Following a calf injury, it may be hard or impossible to continue activity. The person may even have trouble walking with a normal gait, getting up from a seated position, or going up and down stairs.
Bruising and discoloration can be seen along the back of the calf and occasionally, most common with the more severe cases, there may be bruising along with palpable defects, such as muscle lumpiness, under the skin. These defects can be felt and seen with contraction.
-
Like with most musculoskeletal injuries, a patient history and physical exam performed by a healthcare professional will lead to an accurate diagnosis for acute calf injuries.
A clinician may determine the severity of the calf tear (grade 1 to 3) according to pain and physical limitations, including weakness and loss of motion. These findings may help estimate when a patient can return to activity.
Calf tears can be graded by severity:
Grade 1 is a strain of the muscle fibers
Grade 2 is a partial tear of the muscle
Grade 3 is a complete tear of the muscle
The diagnostic process will include a patient interview and physical exam but rarely requires medical imaging.
-
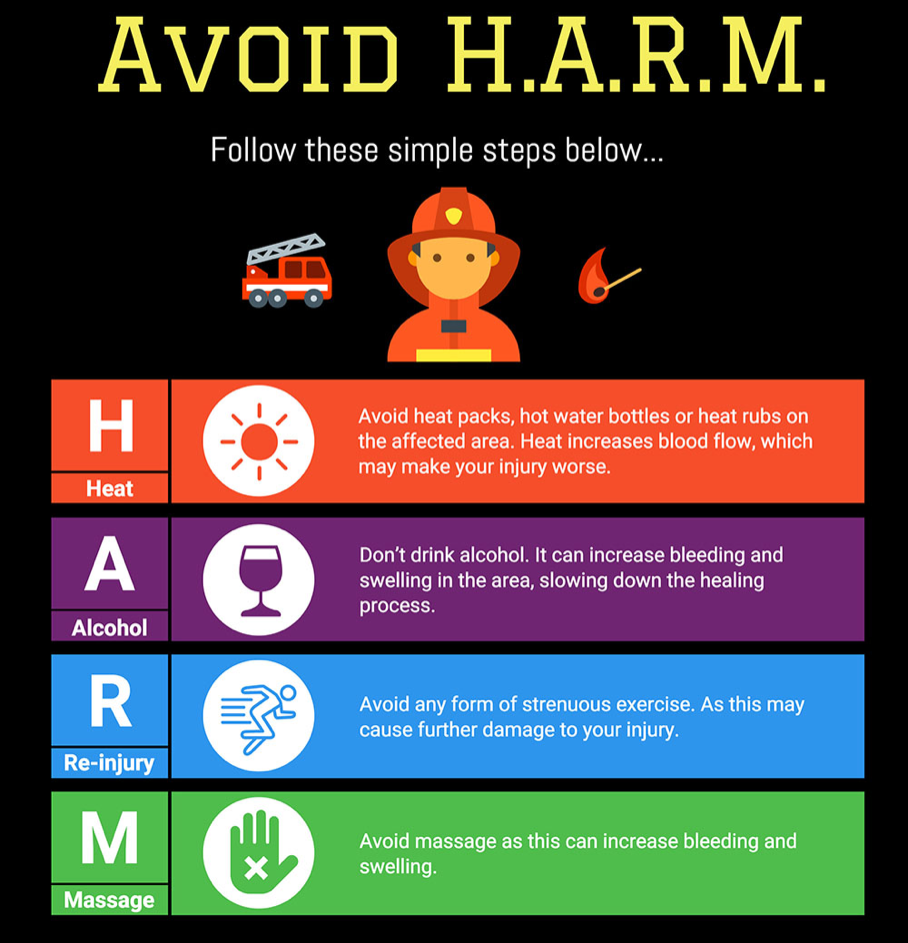
Following a calf muscle strain the main goals are to reduce pain, decrease swelling and protect the affected area from further injury. Previously we used RICE (Rest, ICE, Compression, Elevation) for injury management. However, rest can be harmful and inhibits recovery. Recent research has now advised we use the acronym POLICE
Protection
Optimal-Load
Ice
Compression
Elevation
The key term is Optimal-load, this replaces Rest.
Modifying your normal activities, by reducing prolonged activities on your feet is a form of optimal loading.
Certain taping or strapping can also help to protect the calf muscle and allow you to optimally load the lower leg and ankle without aggravating your symptoms.
You can maintain your fitness using other forms of exercise that will not aggravate your calf, such as swimming, cycling or aqua jogging. You may need to speak to your physiotherapist to discuss what your optimal load might be as it is specific to you but will help speed up your recovery process.
-
It can be difficult to know when to start performing rehab exercises, especially when pain is present which can lead to fear avoidance behavior. As recurrence rates are high, patients often present with a lack of confidence in their ability (self-efficacy) to perform certain exercises or activities during rehabilitation due to fear of re-injury. You can discuss this with your healthcare professional to help maintain your motivation levels thus ensuring you return to normal activities and sport as soon as possible.
“If your injury is very acute it is now recommended NOT TO TAKE ANTI-INFLAMMATORY MEDICATIONS FOR THE FIRST 72 HOURS POST INJURY, as this can affect the tissue healing. Other precautions post-acute injury are shown below.”
Phase 1: Inflammatory phase
During the initial inflammatory phase of healing, the goal should be to control pain, decrease inflammation, and protect the muscle/tendon so scar tissue can develop. This stage may require crutches and taking weight off the injured leg in order to facilitate recovery, healing, and protection. You can gently move the ankle and knee as pain allows.
Avoid excessive stretching during this stage, because it may be detrimental to the recovery process.
The length of this phase depends on the severity of injury, but typically lasts 3 to 7 days. A qualified clinician should make decisions about progression to the next phase based on the patient’s clinical examination and function.
Level One - Strength (Muscle Activation)
It is also normal to experience pain when completing the exercises, however this should not exceed 4/10 on a scale where 0 = no pain and 10 is the most severe pain you could imagine. By using this exercise program it will ensure a quick return to normal activity and sport, whilst reducing the risk of re-injury.
Isometric plantar flexion with band
Repeat each exercise 30 - 60 secpreforming 3 sets - 6 Sets
Isometric double leg heel raise over step in neutral, leg straight and bent
Repeat each exercise 30 - 60 secpreforming 3 sets - 6 Sets
Isometric double leg heel raise over step in neutral, leg straight and bent
Repeat each exercise 30 - 60 secpreforming 3 sets - 6 Sets
Function
Foot Intrinsics/Unstable Surface
(balance on one leg/turn head/pass ball around you) 1 minute x 5
ROM
Ankle Alphabet
Mini squat for ankle movement
Repeat each exercise 12 -15 times preforming 3 sets
Mini Squat for Ankle Movement
Repeat each exercise 12-15 times preforming 3 sets
Level Two - Strength (Muscle Activation)
Double leg heel raise (Body weight), leg straight and bent
Repeat each exercise 15-24 times preforming 4 sets
Seated Heel Raise
10 x 4 @ e.s. 12RM
Function
Isometric Soleus Strength in Split Squat Stance
Repeat each exercise for 30 seconds preforming 6 sets
Rom - Jog - Run
Penguin Steps
Repeat each exercise for 10-20m preforming 3-6 sets
A/B Skips
Repeat each exercise for 10-20m preforming 3-6 sets
Level Three - Strength (Muscle Activation)
Double Leg Heel Raise Over Step
Repeat each exercise 15 -25 times preforming 3 sets
Single leg HR (smith machine)
8 x 4 >70% BW
Seated Heel Raise with Eccentric bias
8 x 4 >120% BW
Function
Pogo Hops in Place
Repeat each exercise 10 times preforming 3 sets
Rom - Jog - Run
Run (gradual build up volume) 4 – 6 x 30 sec run @ 75% of your perceived maximum
Level Four - Strength (Muscle Activation)
SL Eccentric Heel Raise (over step)
8 x 4 >120% Body Weight
If you have access to gym equipment gradually progress to
Sled/Prowler march
100% Body Weight
Sled runs : 60 – 80% Body Weight : lower the weights in the previous drill and increase your speed.
Single leg eccentric heel raise : 8 x 4 140% Body Weight
Function
Ladders
Hurdles
Box Jumps
Repeat each exercise 12 times preforming 4 sets
Stadium Jumps
Repeat each exercise 12 times preforming 4 sets
ROM → Jog → Run
Fly’s 30m 3 – 4 x @ 80 – 90 %
Gradually progress to Accelerations 15 – 20m 4-5 x 80 – 100%
Fly’s 40m 5 – 6 x 90 -100%
C. V.
Maximal aerobic speed (MAS) 6 mins x 2 (30:30)
Level Five
Participate in on field session 75 – 100%